A subscription to JoVE is required to view this content. Sign in or start your free trial.
Surgical Closure of Equine Abdomen, Prevention, and Management of Incisional Complications
In This Article
Summary
This paper describes a method of abdominal wall closure using tension and apposition sutures in horses undergoing ventral midline laparotomies. It also describes methods for prevention and management of postoperative incisional complications, such as bandaging, negative pressure therapy, and in case of wound breakdown, the application of retention sutures.
Abstract
Although rarely fatal, complications of ventral midline laparotomy incision in equine patients increase hospitalization cost and duration and may jeopardize return to athletic function. Therefore, many techniques have been developed to reduce their occurrence and expedite their resolution when they occur. Our technique of celiotomy incision closure includes the use of tension sutures (vertical U mattress) of polyglactin 910 on the linea alba, which is then apposed by polyglactin 910 interrupted sutures or a simple continuous pattern suture with a stop midway before routine closure of the superficial layers. The celiotomy incision is protected by an elastic bandage during the immediate postoperative period. This technique has been associated with favorable results: 5.3% confirmed incisional infections after a single celiotomy and 26.7% after repeat celiotomy. The overall incisional complication (serous/sanguineous discharge, hematoma, infection, hernia formation, and complete wound breakdown) occurrence was 9.5% and 33.3% after single and repeat laparotomy, respectively. In cases considered more susceptible to infection (early relaparotomy or laparotomy incisions longer than 30 cm), negative pressure therapy was found easy to apply on closed incisions. No detrimental effects were observed. However, the potential prophylactic benefit of this therapy needs to be confirmed in a larger group. In infected laparotomy wounds requiring drainage, the use of negative pressure therapy seemed to have a positive effect on the formation of granulation tissue. However, there was no control group to allow statistical confirmation. Finally, one case of complete breakdown of the laparotomy incision was managed by stainless steel retention sutures, the application of negative pressure therapy, and a hernia belt. At re-evaluation 15 months post-surgery, several small hernias were detected, but the horse had returned to his previous level of sports performance and had not shown any episode of colic.
Introduction
The ventral midline celiotomy is the most frequent surgical approach to the abdomen in horses with acute colic1 or in need of cesarean section2. The created ventral incision may be the site of several postoperative complications, such as (sero) sanguineous discharge, infection, hernia formation, and complete wound breakdown3. Except for the case of complete wound breakdown, laparotomy incision complications are rarely fatal, but they increase hospitalization duration and costs and may prevent return to athletic function4,5.
Among incisional complications, infection should be considered one of the most clinically relevant, as its prevalence ranges from 2.7% to 40%6 and can be as high as 68.4% after early repeat laparotomy7. Furthermore, incisional infection is considered a major risk factor for subsequent hernia formation8. Therefore, for several decades, many efforts have been made to reduce the occurrence of incisional infections and expedite their resolution when they occur.
Several techniques of closure of the equine abdomen have been described5. Overall, the linea alba is most frequently closed with a simple continuous pattern, mainly because of its even distribution over the entire incision line, its fast application, and a generally good outcome5,9. However, the closure of the linea alba in an interrupted pattern has also been associated with good results3,10. The subcutaneous and cutaneous tissues may be closed by multiple patterns and with different types of material4,5,11.
In many equine hospitals, postoperative abdominal bandages are now routinely used to protect and provide some support to incision1. Several types of bandages have been described, including elastic bandages and commercially produced hernia belts12, but the actual types of bandages and timing of placement reported in the literature are sometimes unclear.
Despite all the prevention methods used, incisional infection may occur. In these cases, staples or sutures need to be removed in order to evacuate the purulent material and create a ventral drainage for large subcutaneous pockets. Frequent wound cleaning and removal of secretions are indicated to allow the wound to heal by the second intention. Abdominal bandages are particularly encouraged in infected cases for support and to decrease the risk of dehiscence or stretching of the weakened abdominal wall6.
For more than 25 years, negative pressure wound therapy (NPWT) has been used for the treatment of open wounds in human13 and animal patients14. Recently, negative pressure therapy has been investigated as a possible prophylactic measure to prevent complications via immediate application after surgery in high-risk, clean, closed surgical incisions and showed encouraging results15,16. The reported properties of NPWT are wound environment stabilization, wound edema/bacterial load reduction, improved tissue perfusion, as well as granulation tissue, and angiogenesis stimulation13. The management of abdominal wound dehiscence with negative pressure therapy has shown successful results in human patients with compromised healing17. In the rare cases of complete acute or delayed breakdown of the incision in horses, the abdominal wall should be closed with interrupted through-and-through stainless steel retention sutures, and the skin incision left to heal by second intention18. Encouraging results in human medicine suggest that negative pressure therapy could be used as part of the management of dehiscence cases in equine patients, as well as any infected incisional wound, which to our knowledge has not been reported yet.
The aim of this paper is to describe our technique of closure of the equine abdomen with an interrupted pattern using a combination of tension and apposition sutures on the linea alba and our postoperative protocol. This includes abdominal bandaging and, in some cases, the use of negative pressure therapy for the prevention and treatment of incisional complications. Our technique for management of delayed breakdown of the incision is also presented.
Protocol
This retrospective study is based on our clinical records. Our practice fully respects the animal care guidelines of our institution, the Equine Clinic of the University of Liège. Animals included in the study were horses and ponies (mares, intact and gelded males) of various breeds (mainly Warmbloods), of various ages (from 5 months to 34 years, with a mean age around 10 years) and of various weights (from 50 kg to 840 kg, with a mean weight around 500 kg).
1. Surgical technique (ventral midline laparotomy for colic or C-section)
- Surgical preparation and incision
- Preoperatively, administer intravenous (IV) sodium penicillin (20,000 IU/kg), gentamicin (6.6 mg/kg or 8.8 mg/kg), and flunixin meglumine (1.1 mg/kg) +/- subcutaneous enoxaparin (150 mg/500 kg of bodyweight) to the horse.
- After induction of general anesthesia, place the horse in dorsal recumbency.
NOTE: Confirm proper anesthetization by recumbency and the decrease of palpebral reflex. Administer polymer eye ointment to prevent dryness of the cornea during anesthesia. - Trim the abdominal hair and shave a 10 cm wide band centered on the linea alba. In males, wash the penis and sheath with 3.75% povidone-iodine soap or 4% chlorhexidine digluconate soap until visually clean. Then grossly clean the abdomen with 3 cycles of 3.75% povidone-iodine soap or 4% chlorhexidine soap and rinse with tap water.
- Place a urinary catheter. For males, after placement of a stack of 4 inch x 4 inch gauze pads, close the prepuce using Backhaus towel clamps.
- Prepare the abdomen aseptically with a 5 min scrub with 3.75% povidone-iodine or 4% chlorhexidine soap, and rinse after the last cycle with 70% isopropyl alcohol. Finally, spray a 3% povidone-iodine in isopropyl alcohol solution on the surgical site i.e., ventral abdomen, centered on the linea alba.
- Double drape the abdomen: place an iodophor adhesive film on the intended surgical site and drapes from a universal pack around. Then, cover them with a laparotomy drape with incise film on its center.
NOTE: For C-section, place additional drapes. These will be removed once the foal has been extracted and the uterus is closed. - Perform the ventral midline laparotomy cranial to the umbilicus, as routinely done. If required by surgical procedures, extend the (15-20 cm initial) incision further cranially and/or caudally. Perform hemostasis by the application of hemostatic forceps.
- During surgery, repeat intravenous sodium penicillin (20,000 IU/kg) every 90 min.
- Closure of the abdomen
- Change surgical gloves. Dissect the subcutaneous tissue over a width of 1-2 cm along the incision.
- Tension sutures: Preplace (but do not immediately tighten) a series of vertical U mattress sutures (6 metric polyglactin 910) 3 cm apart on the muscular layer.
- To do so, place the far-far loop approximately 1.5 cm from the linea alba incision and the near-near loop at approximately 0.5 cm from the incision. Ensure that retroperitoneal fat and peritoneum are excluded from the sutures. Keep each suture with long strands and place a hemostatic clamp on both strands of each suture.
- When all sutures are preplaced, hold them under tension by an assistant and knot each of them separately.
- Apposition sutures to obtain a tight closure of the linea alba: place interrupted sutures (usually a combination of simple, cruciate, and/or inverted cruciate sutures; 2 and/or 6 metric polyglactin 910) in between the vertical mattress sutures. At the end of this step, check the tightness of the closure with the closed tip of a needle holder: it can no longer pass through the incision.
NOTE: Alternatively, tight closure of the linea alba can be reached using a simple continuous pattern (6 metric polyglactin 910), interrupted 1 or 2 times (depending on the length of the incision) applied on the linea alba over the vertical mattress sutures. - Rinse the incision with 1 L of saline and remove all blood clots with gauze.
NOTE: The rinsing solution may contain 20 mL of 10% gentamicin, depending on the surgeon's preference. - Close the subcutaneous tissue with a simple continuous pattern (0 metric polyglecaprone, cutting needle). In the case of long incisions (i.e., C-section), interrupt the continuous pattern at mid-length.
- Apply staples on the skin at every 5 mm.
- Apply a moisture vapor permeable spray dressing over the incision. Then, cover it with sterile gauze. Cover the ventral abdomen with a non-iodophor adhesive drape.
- Immediately on arrival in the recovery stall, hoist the horse and place an abdominal bandage over the adhesive drape. To do so, with the help of an assistant, place a Gamgee cotton over the incision and roll elastic adhesive bands over it and around the abdomen. Finally, apply tape over the elastic band at the cranial and caudal parts of the bandage.
- Place the horse on the floor in lateral recumbency and assist the recovery by chemical restraint and the use of head and tail ropes. Keep the horse under constant surveillance until it is standing and able to walk to its intensive care stall.
2. Routine postoperative protocol (if no complication occurs)
- Management of surgical incision
- Standard abdominal bandage
- Immediately after the recovery from anesthesia, move the horse to a stall in the intensive care unit and remove the entire bandage (including the adhesive drape). Inspect the surgical site and evacuate any subcutaneous blood accumulation by applying gentle pressure using your fingers on the incision.
- Apply a new abdominal bandage: with the help of an assistant, place a Gamgee cotton covered by a layer of antiseptic ointment (containing silver sulfadiazine or nitrofurantoin) in contact with the ventral incision, and 2 rolled Gamgee cotton pads on each side of the dorsal spine (for prevention of pressure sores). Roll elastic adhesive bands around the abdomen. Finally, apply tape over the elastic band at the cranial and caudal parts of the bandage.
- Remove the ventral part of the bandage every 2-3 days. Inspect and palpate the incision. In case of doubt about the soundness of the incision, perform an ultrasonography. Then, place a new Gamgee cotton with an antiseptic ointment over the incision and new elastic bands around the abdomen and over the remaining part of the previous bandage.
- On day 10-11 postoperatively, remove the skin staples after aseptic preparation of the site. Apply a last bandage for 3-5 days. Then, remove this bandage entirely with the help of a liquid adhesive remover (in order to reduce skin irritation).
- Use of negative pressure therapy on a closed incision (alternative to standard bandages)
NOTE: Case selection: The negative pressure therapy is applied over closed incisions that are considered more at risk of developing complications, such as long laparotomy incisions (> 30 cm) for colic surgery or C-section and the incisions of early repeat laparotomies (which are performed through the initial incision).- As soon as the horse is standing steady after recovering from anesthesia, move it to an intensive care stall and tie it up. Remove the entire bandage (including the adhesive drape). Inspect the surgical site and evacuate any blood accumulated subcutaneously by digital pressure on the incision. Apply a thin layer of sterile antiseptic gel (Polyaminopropyl Biguanide) over the incision.
- Apply the negative pressure bandage according to the recommendations of the manufacturer. Measure the length of the incision with the help of a sterile paper ruler (provided in the specific kit). Spray the ventral abdomen with an adhesive spray while the surgical incision is protected by sterile gauze. Then, remove the gauze and leave the glue to pause for approximately 2 min.
- Cut the specific foam dressing of the kit 5 cm longer than the length of the surgical incision. Remove the protective film numbered 1 from the foam dressing. Cut 2 small hydrocolloid strips (also provided in the kit) to adapt the width of the dressing and apply them on the cranial and caudal extremities of the dressing on the side that will be in contact with the skin.
NOTE: Note that the lateral borders of the dressing already have these hydrocolloid strips. - Apply the negative pressure dressing over the surgical incision, with the white tissue side of the dressing in contact with the skin and the purple foam outside. Remove the protective films numbered 2 from the foam dressing.
- Remove the central protective layer numbered 1 on the adhesive drape to expose the adhesive side. Apply the drape over the foam dressing on the ventral abdomen of the horse. Peel the lateral protective layers numbered 1 and pat the drape on the skin to form a seal. Remove the external protective layer numbered 2, and finally, remove the perforated blue handling tabs from the extremities of the drape.
- Apply and slightly overlap several adhesive drapes on the ventral abdomen of the horse to cover the entire dressing and contact the surrounding intact skin over at least 7 cm in all directions to form a seal. Repeat step 2.1.2.5 for each additional drape.
- Pinch the adhesive drapes facing the center of the foam and create a hole of 2 cm diameter with scissors or a scalpel blade by removing the piece of drape. Remove protective layers numbered 1 on the pad and apply it with the pad opening in the central disc directly over the hole in the drapes. Peel protective layer numbered 2. Pat the central disc for adhesion and pull back the external blue tab.
NOTE: It is important to create a hole (and not a slit) large enough to avoid the presence of the remaining parts of the adhesive drape to be in contact with the pad opening. Otherwise, the system will get obstructed. - Suspend the negative pressure therapy machine above the horse and protect the electric cables (also placed above the horse) with isolating foam polyethylene sheaths. Insert the canister into the machine. Connect the pad tubing to the canister tubing.
NOTE: The isolating foam polyethylene sheaths can optionally be covered with tar to prevent the horse from chewing them. - Turn the machine ON. Set the negative pressure at -125 mmHg, on a continuous mode. Check the correct functioning of the negative pressure therapy, which is confirmed by the flattening of the foam facing the wound, the achievement of the desired negative pressure, and the absence of an audible alarm.
NOTE: If leakage is detected, it needs to be identified and patched with additional adhesive drapes until vacuum restoration. In case of obstruction of the system, check all connections, and if the problem remains, remove the adhesive drapes and the pad and replace them with new ones. - When the system is correctly working, apply an abdominal bandage, which is similar to the standard bandage described in step 2.1.1.2. with two exceptions: 1) it does not contain any antiseptic ointment on the ventral Gamgee cotton and 2) a supplemental Gamgee cotton is applied underneath the tubing where it is still close to the horse abdomen, to avoid pressure sores. Keep the horse tied up all the time while on negative pressure therapy.
- Remove the negative pressure bandage after 2-3 days. Check the wound while carefully respecting aseptic conditions and place a new negative pressure bandage for 2-3 additional days. Thereafter, definitively remove the negative pressure bandage and replace it with a standard bandage (see step 2.1.1.2.). Follow the steps previously described in 2.1.1.3 and 2.1.1.4. for the remaining part of the incision management.
- Standard abdominal bandage
- Postoperative treatments
- In addition to intravenous fluid therapy, administer postoperative treatments, which consist of IV gentamicin (6.6 or 8.8 mg/kg every 24 h) and penicillin (20,000 IU/kg: either sodium penicillin IV every 6 h or procaine penicillin intramuscularly [IM] - every 12 h) for 5-7 days; non-steroidal anti-inflammatory drugs (flunixin meglumine 1.1 mg/kg IV every 12 h) for 4-5 days and enoxaparin (150 mg/ 500 kg bodyweight subcutaneously every 24 h) for 3 days.
NOTE: The duration of the postoperative treatments and the addition of other treatments (such as prokinetic drugs, supplemental analgesics, oxytocin, etc.) need to be adapted for each animal, taking into account the animal's evolution and the potential presence of complications.
- In addition to intravenous fluid therapy, administer postoperative treatments, which consist of IV gentamicin (6.6 or 8.8 mg/kg every 24 h) and penicillin (20,000 IU/kg: either sodium penicillin IV every 6 h or procaine penicillin intramuscularly [IM] - every 12 h) for 5-7 days; non-steroidal anti-inflammatory drugs (flunixin meglumine 1.1 mg/kg IV every 12 h) for 4-5 days and enoxaparin (150 mg/ 500 kg bodyweight subcutaneously every 24 h) for 3 days.
- Rehabilitation
- Strictly confine the horse to a stall for 10 days. Work on the following recommendations for rehabilitation: 8 weeks of stall rest with hand walks (1-2 times a day, starting from 10 min to 30 min at the end of the recovery period) before exercise or pasture turnout can progressively be resumed.
NOTE: During the last 4 weeks of rest and hand walking, a protocol of exercises adapted from Holcombe et al.19 and Clayton20 can be used. This is optional and left at the discretion of the owner/rider.
- Strictly confine the horse to a stall for 10 days. Work on the following recommendations for rehabilitation: 8 weeks of stall rest with hand walks (1-2 times a day, starting from 10 min to 30 min at the end of the recovery period) before exercise or pasture turnout can progressively be resumed.
3. Management of infection over the entire length of the incision by a negative pressure therapy
NOTE: Clinical signs for which to perform this: Incisional purulent or sero-purulent discharge, incisional tenderness with subcutaneous fluid pocket along the incision (detected by ultrasonography), and collection of purulent material when this liquid is aspirated (with needle and syringe).
- If necessary (presence of hairs longer than a few mm), shave the skin around the incision. After aseptic preparation, re-open the skin and subcutaneous tissues to drain the secretions. Perform a bacteriological culture and sensitivity test either by swabbing the depth of the infected incision or by collecting the purulent material with a sterile needle and syringe before opening the skin and subcutaneous tissues.
- Debride the wound: Remove any infected tissue or biofilm by curettage and flush with a sterile isotonic solution. Apply a thin layer of sterile 0.1% polyaminopropyl biguanide gel on the cleaned wound.
- Apply the negative pressure bandage according to the recommendations of the manufacturer. Measure the length of the incision with the help of a sterile paper ruler. Apply an adhesive spray on the ventral abdomen while the open wound is protected by sterile gauze. Then, remove the gauze and leave the glue to pause for approximately 2 min.
- Cut a piece of silver foam to the exact dimensions of the wound and place this foam on the wound and inside the cutaneous rims. Make sure that the foam does not overlap intact skin.
- Follow the next steps of the placement of the negative pressure bandage as previously described (steps 2.1.2.5. to 2.1.2.10.).
- Place an abdominal hernia belt (without additional ventral reinforcement, but with the thick dorsal foam pad) over the elastic bandage to prevent/reduce the risk of abdominal hernia formation. Note that a breast collar is rarely necessary.
- Change the negative pressure therapy bandage every 3-4 days. At each bandage change, perform a debridement of the wound (if needed) and remove any very loose suture material.
NOTE: It is important to avoid letting the same foam come in contact with the wound for longer than 5 days because granulation tissue will grow inside the small holes of the foam, causing difficulties in removing the foam and bleeding after foam removal. - Continue the negative pressure therapy until almost all the abdominal incision is covered by granulation tissue. This usually takes no more than 2 weeks.
- When the negative pressure therapy is stopped, let the horse carry out free movements in the stall. Provide daily wound care (debridement and removal of the secretions).
- On the first day, place a standard elastic abdominal bandage (see step 2.1.1.2.) covered by a hernia belt (and dorsal foam). For the next days, after removal of the ventral part of the abdominal bandage and the wound cleaning, only cover the wound with a Gamgee cotton with antiseptic ointment (hold in place with a few stripes of large tape) and the hernia belt. This lighter bandage reduces the cost of numerous elastic bands. The hernia belt brings some support and protection to the wound.
- Adapt the duration or the type of medical treatments (antimicrobial and non-steroidal anti-inflammatory drugs) to the wound evolution (usually ~ 10-15 days).
- Work on the following recommendations:
- Strict stall rest until complete wound healing (with wound care and hernia belt support - see step 3.9).
- Up to 1 month of stall rest and wearing of the hernia belt without additional ventral reinforcement (which is a curved plastic piece to be placed in the ventral pocket) with daily walks: starting with 5 min of walk per day during the first week, with 5 min increment with every additional week.
- The following month, the horse continues to wear the hernia belt, but the curved plastic piece (with the convex aspect towards the abdomen) is placed in the ventral pocket of the hernia belt. The stall rest is continued, but the frequency of the walk sessions progressively increased to 3-4 times a day. During this month, a program of exercises adapted from Holcombe et al.19 and Clayton20 is recommended.
- After this period, the horse can progressively resume all activities (light work, pasture turnout) if there is no significant abdominal hernia.
NOTE: When the infection is localized to a small area without involving the entire length of the incision, negative pressure therapy can be instituted on the smaller open wound or can be avoided (left at the surgeon's preference). If the negative pressure therapy is not used, local care (as in step 3.2) is performed every day, and the bandage is the same as in step 3.9.
4. Management by retention sutures for subacute breakdown of the incision secondary to severe infection
NOTE: Clinical signs for which to perform this: Severe infection of the entire incision, with loosening of the sutures on the linea alba, gap formation in the linea alba incision allowing the introduction of one or more fingers through it, and abnormally large quantities of fluid (i.e., 300 mL/day) draining in the bandage or aspirated in the negative pressure therapy canister.
- Surgical preparation and technique
- Give the horse preoperative broad-spectrum antibiotics (based on previous culture and sensitivity), flunixin meglumine (1.1 mg/kg IV), and subcutaneous enoxaparin (150 mg/500 kg of body weight). Protect the infected laparotomy incision with an abdominal bandage. After induction of general anesthesia, place the horse in dorsal recumbency.
NOTE: If sodium penicillin is used, repeat it every 90 min. - Place a urinary catheter. For males, after placement of a stack of 4 inch x 4 inch gauze pads, close the prepuce using Backhaus towel clamps.
- Prepare the abdomen aseptically, around the incision, scrub for 5 min scrub with 3.75% povidone-iodine or 4% chlorhexidine digluconate soap, and rinse only at the end with 70% isopropyl alcohol. Finally, apply 3% povidone-iodine in isopropyl alcohol solution spray. On the infected incision, scrub for 5 min with 0.5% dermic povidone-iodine.
- Double drape the abdomen, place an iodophor adhesive film on the intended surgical site, and drapes from a universal pack around. Then, cover them with a laparotomy drape with incise film on its center.
- Remove all remaining sutures on the linea alba. Perform a new bacteriological culture on the wound. Remove all infected tissues by sharp dissection (removal of the edges of the previous incision of the linea alba) and the liquid material (blood, etc.) using a surgical aspirator. Cautiously dissect potential adhesions between the bowels and the infected wound.
- Change gloves and apply new sterile drapes. Rinse copiously the edges of the incision and the abdomen with isotonic sterile electrolytes solution (lactated Ringer solution) at 37 °C while fluids are continuously aspirated.
- Evaluate abdominal viscera and perform adhesiolysis, if needed. Perform omentectomy if the greater omentum has not been removed during the previous surgery. Before closure, fill the abdomen with 5 L of lactated Ringer solution added with 75,000 IU of heparin.
- For the retention sutures, cut several segments of sterile stainless steel cerclage wire of 1 mm diameter at a length of 50-60 cm.
- Preplace them in an interrupted vertical U mattress pattern 3 cm apart through the skin, subcutaneous tissue, and muscular layer while excluding the retroperitoneal fat and peritoneum, using a 14G, 8 cm long needle as a wire passer.
- To do so, place the far suture 5 cm away from the wound edge and the near suture 2.5 cm away from the wound edge. On the opposite side from the future knot, pass the loop of the cerclage wire through a 2.5 cm section of plastic tubing to obtain a buttress effect.
- Once all the cerclage wires are preplaced, preplace several retention sutures of 6 metric polyglactin 910 in between the cerclage wire.
NOTE: This second series of retention suture is placed the same way as the cerclage wire but without the plastic tubing and without the need to use a 14G needle to pass through the tissues as the needle is already attached to the suture thread. - While an assistant keeps all the retention sutures of polyglactin 910 under tension to obtain the apposition of the edges of the incision, knot each of them separately.
NOTE: This step allows an easier apposition of the edges of the incision because cerclage wires are more difficult to manipulate and put under tension the first time. - Then, while all the cerclage wires are kept under maximal tension by 1-2 assistant(s), twist (manually first and then with a pair of flat-nosed pliers) the ends of each vertical mattress separately.
- Cut the ends of each wire with cutting pliers at 3 cm length, then tuck and glue the cut ends of the wires into a section of plastic tubing. Remove the sutures of polyglactin 910. Do not suture the subcutaneous tissue and the skin to allow for drainage.
- Apply a moisture vapor permeable spray dressing over the incision. Then, cover it with sterile gauze. Cover the ventral abdomen with a non-iodophor adhesive drape.
NOTE: The recovery from anesthesia is the same as in steps 1.2.8. and 1.2.9. with the addition of a hernia belt (without additional ventral reinforcement) over the elastic bandage.
- Give the horse preoperative broad-spectrum antibiotics (based on previous culture and sensitivity), flunixin meglumine (1.1 mg/kg IV), and subcutaneous enoxaparin (150 mg/500 kg of body weight). Protect the infected laparotomy incision with an abdominal bandage. After induction of general anesthesia, place the horse in dorsal recumbency.
- Postoperative management
- As soon as the horse is standing steady after the recovery from anesthesia, move it to an intensive care stall and tie it up. Remove the entire bandage, including the adhesive drape. Dry the surgical site with sterile gauze.
- Apply the negative pressure therapy using the procedures described in steps 3.3 to 3.6, with the only difference that the foam is not cut to adapt the dimensions of the wound but covers the ventral incision and the metallic sutures altogether.
- Change the negative pressure therapy bandage the first postoperative day and then every 3-4 days until the edges of the ventral incision are united by a healthy granulation tissue (approximately 8 days).
- When the negative pressure therapy is definitively stopped, let the horse free in the stall. Place a standard elastic abdominal bandage (see step 2.1.1.2.) covered by a hernia belt (and dorsal foam). Change the ventral part of this bandage every 2-3 days for wound care (wound debridement and removal of the secretions).
NOTE: The initial incision is usually not producing most of the secretions. The main secretions come from the abaxial cerclage wires and bolsters that become progressively embedded in granulation tissue. - Remove cerclage wires and bolsters when they no longer provide support because they are cutting through the skin. After aseptic preparation, perform a staged removal by cutting the cerclage wires with cutting pliers on the standing sedated horse (on days 13 and 16).
- Continue the wound care every other day until complete healing of all wounds: the ventral midline wound and the abaxial wounds that occurred secondary to the placement of the cerclage wires. Maintain the standard elastic bandage and the hernia belt.
- Adapt the duration of medical treatments (antimicrobial and non-steroidal anti-inflammatory drugs) to the evolution of the wound (approximately 3-4 weeks).
- Perform rehabilitation as done in step 3.11.

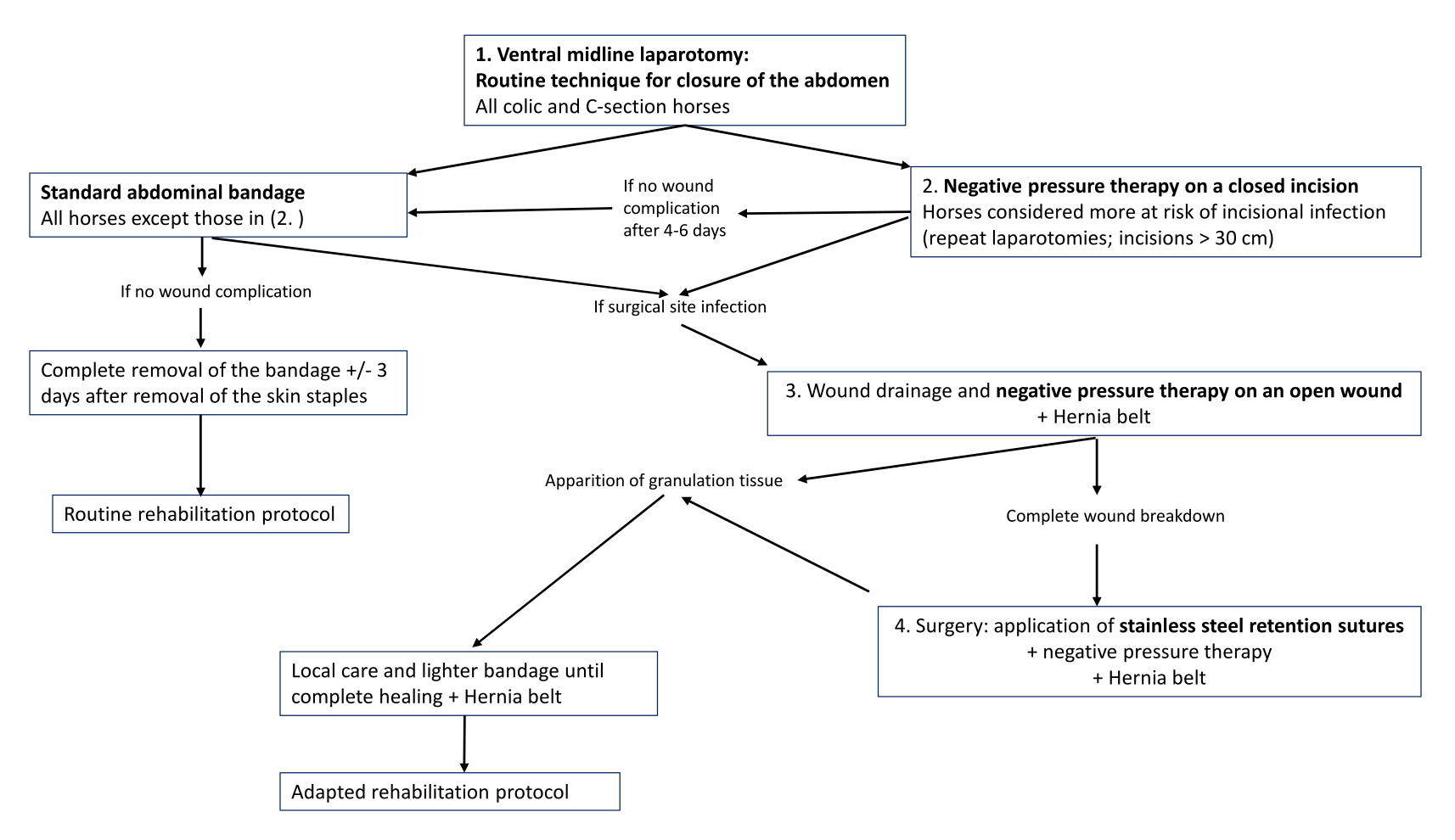
Figure 1: Decision tree. The decision tree for management of laparotomy incisions and their potential complications. Please click here to view a larger version of this figure.
{kind=link}
Results
Routine surgical technique for closure of the abdominal incision and postoperative management: Our technique of closure of the linea alba and routine postoperative management have only undergone minor adaptations since their publication in 20203.
Therefore, for horses operated for abdominal pain, the results presented here are those of this retrospective study³, involving 606 laparotomies performed in 564 horses presenting colic signs during the study...
Discussion
In our clinic, the technique for closure of the equine abdomen is based on a combination of an interrupted vertical U mattress and apposition sutures on the linea alba. In our experience, disadvantages associated with an interrupted pattern suture, such as a greater amount of suture material within the incision and a slower application5, are balanced by several other advantages. Interrupted vertical mattress sutures are particularly indicated for regions under tension and at risk of ...
Disclosures
The authors declare no conflict of interest with any company trading one of the above-mentioned products.
Acknowledgements
The authors would like to thank Ms. Jennifer Romainville and Cyrielle Bougeard for their technical help during procedures and all members of the Clinic (especially the anesthetists, residents in surgery, interns, students, and grooms) for their assistance and care to the patients. The owners of the horse operated with the retention sutures are also thanked for answering the long-term follow-up questionnaire and allowing taking pictures of the horse. Finally, the authors thank M. Laurent Leinartz for his help in editing the pictures.
Materials
| Name | Company | Catalog Number | Comments |
| 300 ml canister (with gel) for ACTIV.A.C. Therapy system | KCI | M8275058/5 M8275058/10 | canister for negative pressure therapy |
| Alfatec 6 HRTX 50 | Prodivet Pharmaceutical produced by Chirina T Injecta | PG0649P | 6 metric polyglactin 910 |
| Appose ULC Slim Body Skin Stapler | Covidien | 88868037 12 | skin staples |
| AquaPharm NaCl 1l | Ecuphar | 366 4174 | 1 L saline |
| Bovivet reinforced disposable needle 14G x 3 1/4'' . 2.1 x 80 mm | Kruuse | 112462 | needle used when placing the stainless steel retention sutures |
| Buster Surgery Cover 120 cm x 180 cm | Kruuse | 141 850 | surgical drapes |
| Clexane 15.000 UI | Sanofi | BE-230185 | enoxaparin |
| CM Hernia Belt | CM Equine Products | Hernia belt: various sizes, to be adapted to the horse's dimensions | |
| Cutting plier 24 cm maxi 3 mm 1456 | Alcyon | 8387671 | cutting plier |
| Dermanios Scrub | Anios | BE-REG-00679 | Chlorhexidine digluconate soap |
| Dermincise 80 cm x 60 cm | Vygon | 38 80 60 | non-iodophor adhesive drape |
| Digital Ultrasonic Diagnostic Imaging System | Mindray | DP-50Vet | ultrasound machine |
| e band | Millpledge | DQ05100 | elastic adhesive roll |
| Ethanol 70% | Savetis | Isopropyl alcohol | |
| Fil de cerclage AO 1 mm x 10 m | Alcyon | 8022030 | 1 mm diameter stainless steel cerclage wire |
| Flammazine 1% creme | Alliance Pharma | BE270505 | silver sulfadiazine dressing |
| Flat-nosed pliers 180 mm | Alcyon | 8368113 | flat-nosed pliers |
| Furacine Soluble Dressing | Limacom nv | BE300876 | nitrofurantoin dressing |
| Genta Equine 100 mg/ml | Divasa-Farmavic | BE-101491 | gentamicin |
| Heparine Leo 5000 U.I./ml | Leo | 1361-559 | heparin |
| Info.V.A.C. | KCI | 413781 Rev B | negative pressure therapy machine |
| Intrafix Primeline | B Braun | 4062182 | plastic tubing (for buttress effect for retention sutures) |
| Ioban 56 cm x 60 cm | 3M | 6648EU | iodophor adhesive film |
| Iso-Betadine Dermicum | Mylan | BE007077 | dermic povidone iodine |
| Iso-Betadine Savon | Mylan | BE007095 | Povidone iodine soap |
| Kruuse adhesive spray | Kruuse | 141865 | adhesive spray |
| Laparotomy Sheet with Incise Film Eclipse | Medline | 29511CEA | laparotomy drape with incise film |
| Leukotape Classic | BSN medical | 01703-00 | adhesive tape |
| Leukotape Remover | BSN medical | 97285-05 | Liquid adhesive remover |
| Meganyl 50 mg/ml | Syva | 4117-446 | flunixine meglumine |
| Monocryl 0 CP-1 | Ethicon | C267 | 0 metric polyglecaprone, cutting needle |
| Opsite | Smith and Nephew | 66004978 | Moisture vapour permeable spray dressing |
| Penicilline 5.000.000 UI | Kela | 7E33729E19 | Sodium Penicillin |
| Peni-Kel 300.000 UI/ml | Kela | 1370-881 | Procain Penicillin |
| Poviderm Sol | Emdoka | BE-V196971 | Povidone iodine in isopropyl alcohol solution |
| Prevena Plus Customizable dressing | KCI | PRE4055 | Kit for negative pressure therapy on closed wounds |
| Prontosan | B Braun | 400 505 | Gel continaing 0,1% Polyaminopropyl Biguanide (polihexanide) |
| Saddle pad (equine size) | CM Equine Products | SP-E1 | large foam pad for protection of the horse's back |
| SENSAT.R.A.C. Pad | KCI | M8275057/10 | Pad with central disc for negative pressure therapy |
| Thilo-Tears | Alcon NV | 233866 | Polymer eye ointment |
| Universal Pack Eclipse | Medline | 29105CEA | universal pack (drapes) |
| V.A.C. Drape | KCI | M6275009/10 | adhesive drape for negative pressure therapy |
| V.A.C. Granufoam silver Dressing | KCI | M8275099/5 M8275099/10 | silver foam for negative pressure therapy |
| Vetivex Ringer Lactate solution 5000 ml | Dechra | BE-V442032 | 5 L Pouch of Lactated Ringer's Solution |
| Vicryl 2 CTX | Ethicon | V367H | 2 metric polyglactin 910 |
| Zorbo-G-Padding | Millpledge | DX05200 | Gamgee cotton |
References
- Marshall, J. F., Blikslager, A. T., JA, A. u. e. r., Stick, J. A., Kümmerle, J. M., Prange, T. Colic: Diagnosis, Surgical Decision, Preoperative Management, and Surgical approaches to the Abdomen. Equine Surgery (5th edition). , 521-528 (2019).
- Woodie, J. B., JA, A. u. e. r., Stick, J. A., Kümmerle, J. M., Prange, T. Uterus and ovaries. Equine Surgery (5th edition). , 1083-1094 (2019).
- Salciccia, A. Complications associated with closure of the linea alba using a combination of interrupted vertical mattress and simple interrupted sutures in equine laparotomies. Vet Rec. 187 (11), e94 (2020).
- Salem, S. E., Proudman, C. J., Archer, D. C. Prevention of post operative complications following surgical treatment of equine colic: Current evidence. Equine Vet J. 48 (2), 143-151 (2016).
- Mair, T. S., Smith, L. J., Sherlock, C. E. Evidence-based gastrointestinal surgery in horses. Vet Clin North Am Equine Pract. 23 (2), 267-292 (2007).
- Fogle, C., JA, A. u. e. r., Stick, J. A., Kümmerle, J. M., Prange, T. Postoperative care, complications, and reoperation of the colic patient. Equine Surgery (5th edition). , 660-677 (2019).
- Dunkel, B., Mair, T., Marr, C. M., Carnwath, J., Bolt, D. M. Indications, complications, and outcome of horses undergoing repeated celiotomy within 14 days after the first colic surgery: 95 cases (2005-2013). J Am Vet Med Assoc. 246 (5), 540-546 (2015).
- Ingle-Fehr, J. E., Baxter, G. M., Howard, R. D., Trotter, G. W., Stashak, T. S. Bacterial culturing of ventral median celiotomies for prediction of postoperative incisional complications in horses. Vet Surg. 26 (1), 7-13 (1997).
- Freeman, D. E., Rötting, A. K., Inoue, O. J. Abdominal closure and complications. Clin Tech Equine Pract. 1 (3), 174-187 (2002).
- Rinnovati, R., Romagnoli, N., Stancampiano, L., Spadari, A. Occurrence of incisional complications after closure of equine ventral midline celiotomies with 2 Polyglycolic acid in simple interrupted suture pattern. J Equine Vet Sci. 47, 80-83 (2016).
- Torfs, S., et al. Risk factors for incisional complications after exploratory celiotomy in horses: do skin staples increase the risk. Vet Surg. 39 (5), 616-620 (2010).
- Canada, N. C., Beard, W. L., Guyan, M. E., White, B. J. Comparison of sub-bandage pressures achieved by 3 abdominal bandaging techniques in horses. Equine Vet J. 47 (5), 599-602 (2015).
- Agarwal, P., Kukrele, R., Sharma, D. Vacuum assisted closure (VAC)/negative pressure wound therapy (NPWT) for difficult wounds: A review. J Clin Orthop Trauma. 10 (5), 845-848 (2019).
- Stanley, B. J. Negative pressure wound therapy. Vet Clin North Am Small Anim Pract. 47 (6), 1203-1220 (2017).
- Dyck, B. A. Use of incisional vacuum-assisted closure in the prevention of postoperative infection in high-risk patients who underwent spine surgery: a proof-of-concept study. J Neurosurg Spine. 31 (3), 430-439 (2019).
- Scalise, A., et al. Improving wound healing and preventing surgical site complications of closed surgical incisions: a possible role of incisional negative pressure wound therapy. A systematic review of the literature. Int Wound J. 13 (6), 1260-1281 (2016).
- Heller, L., Levin, S. L., Butler, C. E. Management of abdominal wound dehiscence using vacuum assisted closure in patients with compromised healing. Am J Surg. 191 (2), 165-172 (2006).
- Toth, F., Schumacher, J., JA, A. u. e. r., Stick, J. A., Kümmerle, J. M., Prange, T. Abdominal hernias. Equine Surgery (5th edition). , 645-659 (2019).
- Holcombe, S. J., Shearer, T. R., Valberg, S. J. The effect of core abdominal muscle rehabilitation exercises on return to training and performance in horses after colic surgery. J Equine Vet Sci. 75, 14-18 (2019).
- Clayton, H. M. Core training and rehabilitation in horses. Vet Clin North Am Equine Pract. 32 (1), 49-71 (2016).
- Weiland, D. E., Bay, R. C., Del Sordi, S. Choosing the best abdominal closure by meta-analysis. Am J Surg. 176 (6), 666-670 (1998).
- Gupta, H., et al. Comparison of interrupted versus continuous closure in abdominal wound repair: a meta-analysis of 23 trials. Asian J Surg. 31 (3), 104-114 (2008).
- Provost, P. J., Bailey, J. V., JA, A. u. e. r., Stick, J. A. Principles of plastic and reconstructive surgery. Equine Surgery (4th edition). , 271-284 (2012).
- Mair, T. S., Smith, L. J. Survival and complication rates in 300 horses undergoing surgical treatment of colic. Part 2: Short-term complications. Equine Vet J. 37 (4), 303-309 (2005).
- Smith, L. J., Mellor, D. J., Marr, C. M., Reid, S. W., Mair, T. S. Incisional complications following exploratory celiotomy: does an abdominal bandage reduce the risk. Equine Vet J. 39 (3), 277-283 (2007).
- Klohnen, A. New perspectives in postoperative complications after abdominal surgery. Vet Clin North Am Equine Pract. 25 (2), 341-350 (2009).
- Freeman, K. D., Southwood, L. L., Lane, J., Lindborg, S., Aceto, H. W. Post operative infection, pyrexia and perioperative antimicrobial drug use in surgical colic patients. Equine Vet J. 44 (4), 476-481 (2012).
- Birke-Sorensen, H. Evidence-based recommendations for negative pressure wound therapy: treatment variables (pressure levels, wound filler and contact layer)-steps towards an international consensus. J Plast Reconstr Aesthet Surg. 64 (Suppl), S1-S16 (2011).
- Jordana-Garcia, M., Pint, E., Martens, A. The use of vacuum-assisted wound closure to enhance skin graft acceptance in a horse. Vlaams Diergeneeskundig Tijdschrift. 80 (5), 343-350 (2011).
- Gemeinhardt, K., Molnar, J. Vacuum-assisted closure for management of a traumatic neck wound in a horse. Equine Vet Edu. 17 (1), 27-33 (2005).
- Salciccia, A., Grulke, S. de la Rebière de Pouyade, G. La ténosynovite septique - 2e partie: traitement et pronostic. Le Nouveau Praticien Vétérinaire - Equine. 16 (56), 20-24 (2022).
- Gaus, M., Rohn, K., Roetting, A. K. Applicability and effect of a vacuum-assisted wound therapy after median laparotomy in horses. Pferdeheilkunde-Equine Medicine. 33 (6), 563-572 (2017).
- Bramlage, L. R., Richardson, D. W., Markel, M. D., von Salis, B., Fackelman, G. E., Auer, J. A., Nunamaker, D. M. Mandible, maxilla and skull. AO Principles of Equine Osteosynthesis. , 34-55 (2000).
Reprints and Permissions
Request permission to reuse the text or figures of this JoVE article
Request PermissionThis article has been published
Video Coming Soon
Copyright © 2025 MyJoVE Corporation. All rights reserved